|
» Back to Table of Contents
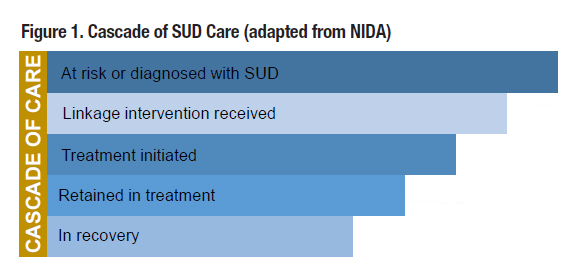 In their lead commentary article, Dr. Drexler and Dr. Burden state the need to treat substance use disorders (SUDs) in the same manner as other chronic diseases by providing a comprehensive management approach that encompasses prevention, identification, early intervention, treatment, and recovery. In agreement, substance use researchers have suggested using the “cascade of care” framework to identify gaps along the continuum of care and to tailor interventions that improve the quality and outcomes of care (Figure 1). The cascade of care has been shown as a useful tool to monitor system-wide effectiveness and performance across the continuum of care for chronic diseases such as HIV and diabetes. Identifying where major gaps occur along the care continuum helps clinicians and researchers design intervention strategies to address them. In their lead commentary article, Dr. Drexler and Dr. Burden state the need to treat substance use disorders (SUDs) in the same manner as other chronic diseases by providing a comprehensive management approach that encompasses prevention, identification, early intervention, treatment, and recovery. In agreement, substance use researchers have suggested using the “cascade of care” framework to identify gaps along the continuum of care and to tailor interventions that improve the quality and outcomes of care (Figure 1). The cascade of care has been shown as a useful tool to monitor system-wide effectiveness and performance across the continuum of care for chronic diseases such as HIV and diabetes. Identifying where major gaps occur along the care continuum helps clinicians and researchers design intervention strategies to address them.
The most prevalent substance use problems among Veterans are heavy episodic drinking and cigarette smoking. In nationally representative samples, 15.1 percent of Veterans had past-year alcohol use disorder (AUD) and 23.1 percent had past-year tobacco use disorder.1 In contrast, 3.3 percent of Veterans had past-year cannabis use disorder, and ≤1 percent had an opioid, cocaine, sedative, or stimulant use disorder.1 Only 28.7 percent of Veterans with a past-year SUD received treatment.1 Of more than 300,000 VHA patients with AUD annually, only about one-third receive treatment in VHA specialty addiction programs.
VHA mandates that all Veterans presenting at primary care clinics receive annual alcohol screening, and that those with a positive screen receive brief counseling. Patients with a positive alcohol screen should be referred to specialty SUD care in those cases when they either have not reduced drinking in response to previous brief counseling, have an AUD diagnosis or a screening score indicating probable AUD, or have co-occurring mental health or medical conditions that can be worsened by alcohol use. As Dr. Drexler and Dr. Burden report, 96 percent of VHA-treated Veterans are screened for at-risk alcohol use, and 84 percent of those with a positive screen receive brief counseling. Brief counseling may be associated with reduced drinking.2 However, among VHA primary care patients identified as engaging in high-risk alcohol use, only about one-third receive advice on alcohol-related treatment options or are offered a psychosocial intervention within 30 days after identification.2 Even lower percentages of Veterans initiate and are retained in AUD treatment when it is offered to them.2 For example, among VHA patients with documented AUD, only 8.5 percent receive any type of approved AUD pharmacotherapy. Significant gaps exist such that more should be done to increase access to and utilization of SUD treatments.
Different care delivery models are needed to offer treatment to Veterans with SUD and increase treatment initiation and retention.3 Substantial barriers exist to linking patients with SUD to treatment, and understanding these barriers is critical to helping clinics and providers identify strategies that may improve linkage. Barriers are well-documented and can be categorized as pertaining to the patient, provider, or care system. Patient-level barriers include not perceiving a need for services, difficulties accessing inconvenient treatments (long wait times, travel distances, inflexible hours), stigma associated with help-seeking, and lack of self-efficacy, motivation, and social support. Provider-level barriers include lack of cultural competence and knowledge about available treatment options, beliefs that addiction treatment is ineffective, and lack of training in SUD treatment. System-level barriers include limited collaboration between care sites.
Research shows that components of referral to treatment (e.g., brief discussions of treatment options, encouraging or prescribing appointment-making, booster sessions) are insufficient in helping patients link to SUD treatment. More intensive yet feasible interventions need adoption to effectively connect patients with SUD to the next care setting.3 Ongoing, supportive contact over time may be needed for patients to recognize and agree that their substance use is problematic and requires behavior change that may be more likely to occur with treatment. An example of such contact delivery is telephone monitoring, which has been shown to decrease repeat detoxifications among Veterans. Another example is delivery of 12-step facilitation interventions that increase Veterans’ involvement in 12-step groups after SUD outpatient treatment, improve patients’ drinking outcomes, and save health care costs. Brief case management also has promise for overcoming potential barriers that interfere with linking patients to SUD treatment, and may be feasible for medical settings such as primary care, pain clinics, or emergency departments with limited time, staffing, and other resources. Brief case management consisting of assessment, planning, monitoring, and advocacy, and teaching patients how to leverage existing skills and strengths to promote treatment linkage, improve initiation of SUD treatment more than motivational interviewing or standard referral. Although possibly requiring more resources to implement, brief case management may help primary care and other settings to overcome patient- and system-level barriers to SUD care.
Two special populations within the SUD cascade of care are women Veterans and Veterans with co-occurring mental health conditions. Although alcohol and drug use disorders are less common among female than male Veterans, between 6 percent to 25 percent of women Veterans screen positive for unhealthy alcohol use (depending on how screening is conducted). Delivering high-quality care to women Veterans requires understanding their specific patterns of substance use and their co-occurring conditions. Most VHA facilities (85 percent) provide women Veterans with SUD-specific individual psychotherapy, but only 30 percent provide SUD-specific women-only groups, and only 14 percent provide SUD-PTSD women-only groups in specialty SUD treatment. At-risk alcohol use and AUD among Veterans are associated with high rates of co-occurring PTSD and depression. Veterans with at-risk alcohol use and co-occurring PTSD or depression are at greater risk for suicide attempts and death, and have greater healthcare utilization and costs, than Veterans without these comorbidities. Alcohol treatment reduces risk of alcohol relapse, hospital admission, and death.
The cascade of care has the potential to help VHA tailor interventions for substance use, evaluate outcomes, and reduce mortality. It provides a basis for accountability and improv- ing individual and population health. Additional research efforts are vital for continued success to fill in gaps along the cascade.
- Boden MT, Hoggatt “Substance Use Disorders Among Veterans in a Nationally Representative Sample: Prevalence and Associated Functioning and Treatment Utilization,” Journal of Studies on Alcohol and Drugs 2018; 79(6):853-61.
- Hepner KA, et “Rates and Impact of Adherence to Recommended Care for Unhealthy Alcohol Use,” Journal of General Internal Medicine 2019; 34(2):256-63.
- Cucciare MA, Coleman EA, Timko “A Conceptual Model to Facilitate Transitions from Primary Care to Specialty Substance Use Disorder Care,” Primary Health Care Research & Development 2015; 16:492-505.
|


